In 2021, the South East London Integrated Care System (SEL ICS) commissioned King’s Health Partners Women and Children's Health (KHP WCH) to deliver "Resilient Health Systems" (RHS) as part of iterative approach to healthcare system design and implementation to facilitate evidence-based decision-making in the health system.
Using a range of evaluation research methods, the project aims to generate and synthesise evidence to guide SEL ICS decision-making. This approach will identify the services, programmes, and policies that enhance the resilience capacities of the health system and, in so doing, allow decision-makers to make evidence-based choices about whether to start, stop, or scale-up innovations.
The RHS project is divided into three phases:
Although Resilient Health Systems (RHS) is a research project, the approach that underpins the collaboration between KHP WCH and SEL ICS is interventional. The Resilient Health Systems Theory of Change highlights how the project is expected to lead to change in the south east London health system.
The project is being delivered by a team of researchers based at King's Health Partners Women and Children's Health
Funders: South East London Integrated Care System
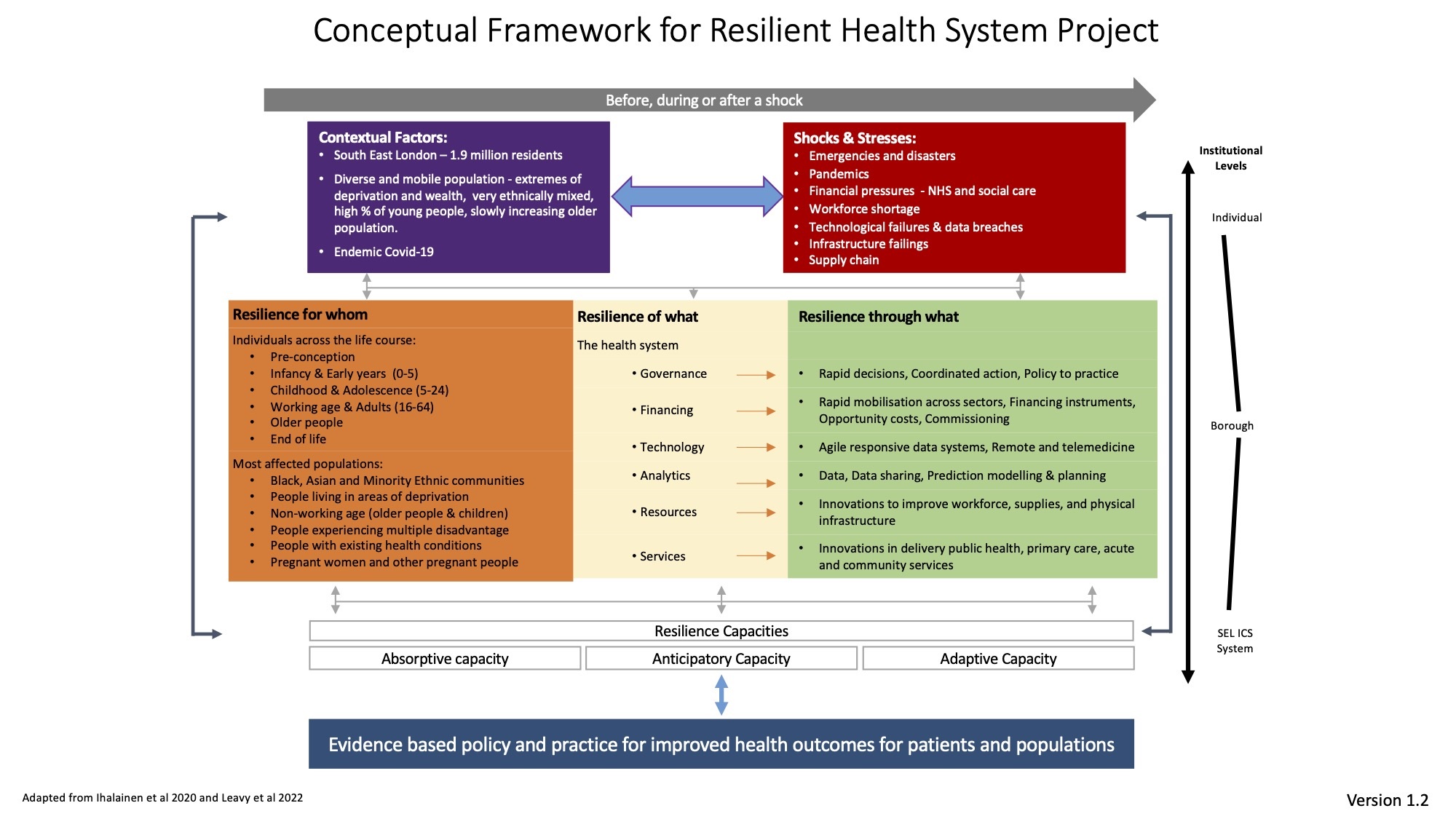
Findings from the scoping and co-design phase of the RHS project indicated that in south east London, the health and social care systems’ ability to bounce back from shocks or absorb ongoing stressors remains precarious. The implementation phase of the RHS project focuses on mapping the resilience capacities of the SEL healthcare system. This phase has been underpinned by the conceptual framework developed during the co-design phase of the project.
The Conceptual Framework represents the complex relationships between various interlinked concepts that influence health system resilience. The framework sets out different pathways and starting points for quantitative and qualitative inquiry and highlights the need for a multi-level approach to analysis. For example, when undertaking a rapid evaluation of an intervention, the resilience framework can be used as a guide to developing the monitoring and evaluation tools. Data collection considers contextual factors, the shocks and stressors of interest, the relevant target populations, interventions, and mechanisms (“resilience for whom, of what and through what”). Data are then synthesised using the framework, for example, by thematically grouping interventions by temporal dimension (before, during or after a shock), resilience capacities, or the targeted level of the intervention.
To date, the RHS project has undertaken:
Aim: understand where, how & why innovations in response to COVID-19 were introduced and understand the resilience capacities of the SEL health system.
Data collection: Five focus groups discussions (FGD) were held with approximately 31 purposively sampled participants. The focus groups covered five of the six domains in the conceptual framework: governance, services, resources, technology, and analytics. It was not possible to conduct a focus group for the finance domain. Participants were given ‘shock’ and ‘stress’ scenarios and asked to discuss the health system’s response. The data was analysed in relation to the resilience capacities outlined in the conceptual framework. This work was presented at the Health Services Research UK conference in July 2023.
Aim: understand where, how and why innovations in response to COVID-19 were introduced and understand the resilience capacities of the SEL health system.
The project team refined and tested the FGD findings by conducting rapid service evaluations of innovative changes to healthcare provision. The evaluated interventions were selected using pre-defined criteria agreed by the RHS project steering committee.
At the King’s Health Partners conference, a workshop was held to start prioritising a set of indicators for health system resilience. The workshop was attended by key informants in KHP and the SEL healthcare system. This is the first step towards a co-designed/produced Resilience Capacity Assessment.
Using the data collected from the focus groups, evaluations, and workshops, the team created a set of recommendations around system resilience, these were presented at the resilience indicator workshop and to the project steering committee and will be developed during the project extension.
The implementation phase currently has three workstreams.
Workstream 1: Developing Resilience Capacity Assessment
A Resilience Capacity Assessment will systematically map and exploring the resilience capacities of any given health or social care system. In the long term, this should lead to stakeholders routinely undertaking such analyses while planning and delivering services. Additionally, in the medium term, the RHS project is expected to lead to the further spread of evidence-based decision-making, with stakeholders across SEL using robust methods to make choices about whether to start, stop or scale-up innovations.
Workstream 2: Refining the Resilience Framework
The framework developed during the co-design phase of the project represents the complex relationships between various interlinked concepts that influence health system resilience. Data from health and policy evaluations will be used to refine the framework so it can be used to design or evaluate interventions to improve system resilience.
Workstream 3: Disseminating Findings
Throughout the project the team will disseminate the findings of the Resilient Health Systems project.
What counts as an innovation or intervention?
We will evaluate ideas, processes, products, or procedures designed to significantly benefit the patients, healthcare professionals or the wider health system. Examples include:
We are keen to evaluate:
We can undertake evaluation research to answer a range of questions including:
We aim to undertake each evaluation rapidly and provide findings within four-six months. Each evaluation follows a simple cycle shown in the figure above.
The RHS project conducts evaluations to benefit those delivering the innovation or intervention. Evaluation findings are often used to:
{kind=link}